Dosing fundamentals: mcg, mg, IU, titration, and cycling
How to read a peptide protocol without getting yourself hurt — units, titration, dose-response, cycling on and off, and why 'more' is almost never 'better'.
The units, plainly
Three units dominate peptide protocols, and confusing them is the single most common rookie mistake — sometimes a dangerous one.
- Microgram (mcg or µg) — one thousandth of a milligram. Most growth-hormone-axis peptides (ipamorelin, CJC-1295, tesamorelin) and PT-141 are dosed in mcg.
- Milligram (mg) — 1,000 mcg. BPC-157, TB-500, semaglutide loading, and most healing peptides are dosed in mg, though individual doses are often hundreds of mcg.
- International Unit (IU) — a standardized biological-activity unit. Used for HGH, HCG, and (separately) as a syringe scale where 1 mL of insulin syringe = 100 IU. Do not confuse the dose unit with the syringe scale — they are unrelated.
A '10' on a U-100 insulin syringe is 10 syringe-IU = 0.10 mL. It is not '10 IU' of the peptide unless you happen to be dosing a peptide measured in IU.
Reading a protocol
A typical line like 'Ipa/CJC 200/100 mcg, 5 nights/week, 8 weeks on / 4 weeks off' unpacks to four things: the dose (200 mcg ipamorelin + 100 mcg CJC-1295 no-DAC), the frequency (5 nights/week — usually weekdays), the cycle length (8 weeks), and the off-period (4 weeks). All four matter. Halving the off-period quietly is the second most common rookie mistake.
Titration: start low, go slow
Every reasonable peptide protocol starts below the published target dose. Two reasons. First, dose-limiting side effects (nausea on GLP-1s, flushing and nausea on MT-II, water retention on GH secretagogues) are real and avoidable with ramps. Second, you cannot attribute a side effect if you start two new compounds at once.
The standard ramp for GLP-1s — semaglutide and tirzepatide — is built into their FDA labels precisely because skipping titration is the difference between 'mild GI upset' and 'in the ER with intractable vomiting'. Treat the ramp as part of the dose, not as a suggestion.
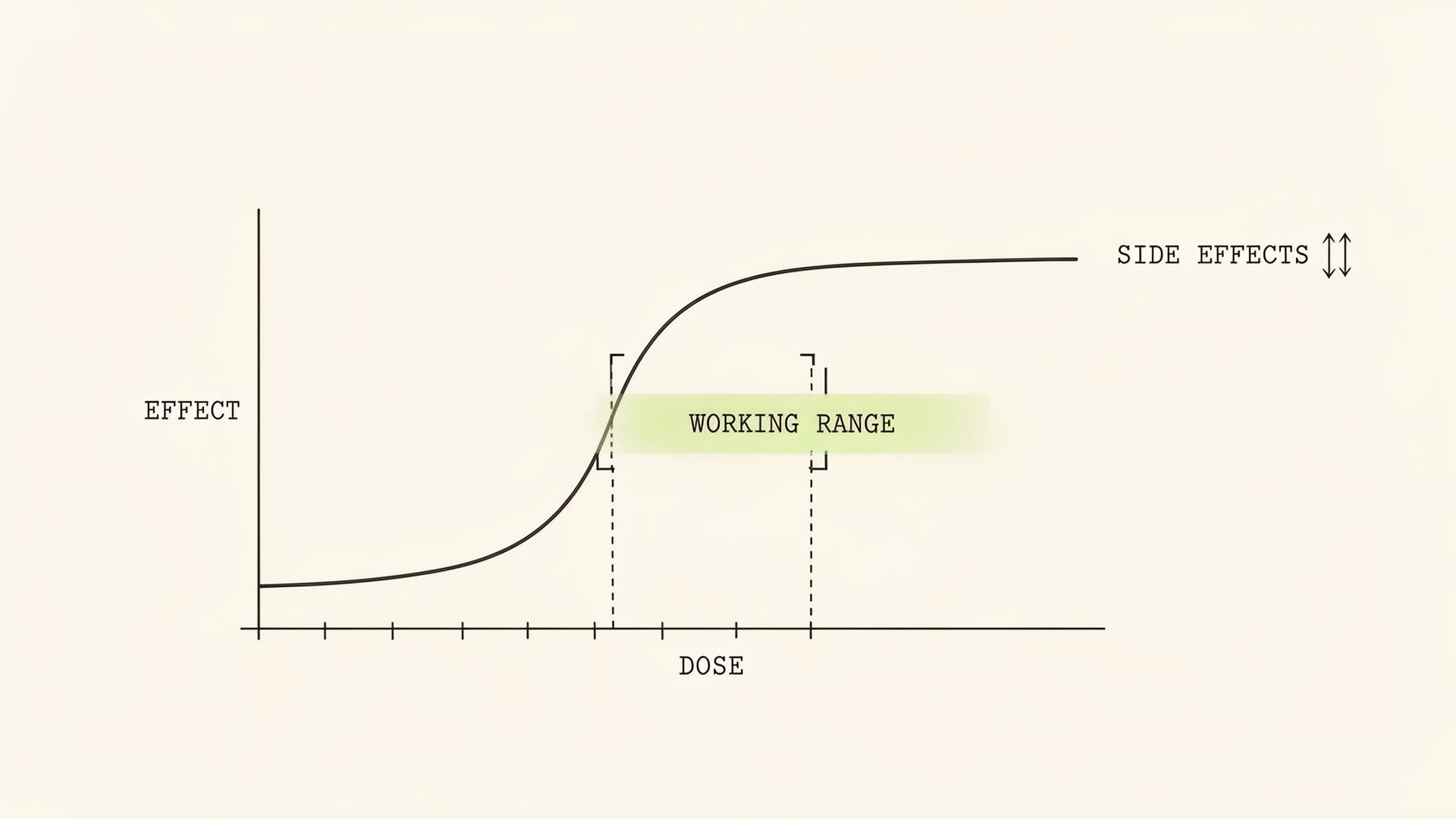
Dose-response is not linear
For most peptides, the dose-response curve is sigmoidal: too little does nothing, the working range is narrow, and beyond the working range you mostly buy side effects. Ipamorelin at 100 mcg and at 300 mcg produce similar GH pulses because the GHSR receptor saturates. Pushing past it gets you appetite, water retention, and sometimes cortisol/prolactin elevation that defeats the point of choosing ipamorelin in the first place.
The correct mental model is: find the bottom of the working range, sit there, and let time do the work.
Cycling: on, off, and why
Cycling exists for two reasons. The first is receptor sensitivity — chronic agonism of any receptor tends to downregulate it (the classic example is melatonin, but the principle applies broadly). The second is signal: an 8-on/4-off cycle lets you tell whether the peptide is doing what you think it is. If you feel identical after the off-period, you have evidence; if you crash, you also have evidence.
Not every peptide needs cycling. GLP-1s are typically taken continuously because the goal is sustained appetite regulation. GH secretagogues are almost always cycled to preserve pulsatility. BPC-157 is usually run for an indication (a specific injury) and stopped, not cycled indefinitely. The Class deep-dives cover each one.
Loading vs maintenance
Some protocols use a higher 'loading' dose for the first 2–4 weeks, then drop to maintenance. This is a useful pattern when you want a quick effect and then steady-state minimum (e.g. some BPC-157 healing protocols, some longevity stacks). It is not appropriate when the goal is appetite regulation or hormonal axis modulation, where steady levels matter more than peak levels.
How not to dose
Patterns we see fail, with depressing regularity:
- Stacking three new peptides on day one. You will have no idea what is doing what — or what is hurting you.
- 'Bro-dosing' — doubling published doses because more must be better. The receptor disagrees.
- Skipping the GLP-1 ramp. The label exists for a reason.
- Running GH secretagogues 7 days a week, indefinitely. You will downregulate, the effect will fade, and you will then conclude the peptide does not work.
- Reusing reconstituted vials past their stability window. You are injecting degraded peptide and possibly bacteria.
How do I convert mcg to insulin units on a U-100 syringe?+
You can't directly — units measure volume on the syringe, not peptide mass. You first need the concentration (mcg per mL) of your reconstituted vial. Use the calculator in the Reconstitution guide, which does the conversion for you.
Why does the package say 5 mg but I dose in micrograms?+
Vial size is the total amount of peptide. Your dose is a fraction of that. A 5 mg vial reconstituted in 2 mL of bac water at a 250 mcg dose gives you 20 doses. The Reconstitution calculator shows this exactly.
Do I need to cycle off every peptide?+
No. The decision is driven by mechanism — receptor desensitization risk, axis suppression risk, and goal. GLP-1s are usually continuous; GH secretagogues are usually cycled; healing peptides are usually run for an indication and stopped.
What is the smallest meaningful dose change?+
On a U-100 insulin syringe, the markings are 2 IU apart at best (some are 1 IU). That is the smallest you can reliably draw at home. If your dose change is smaller than one syringe mark, you are not actually changing the dose.