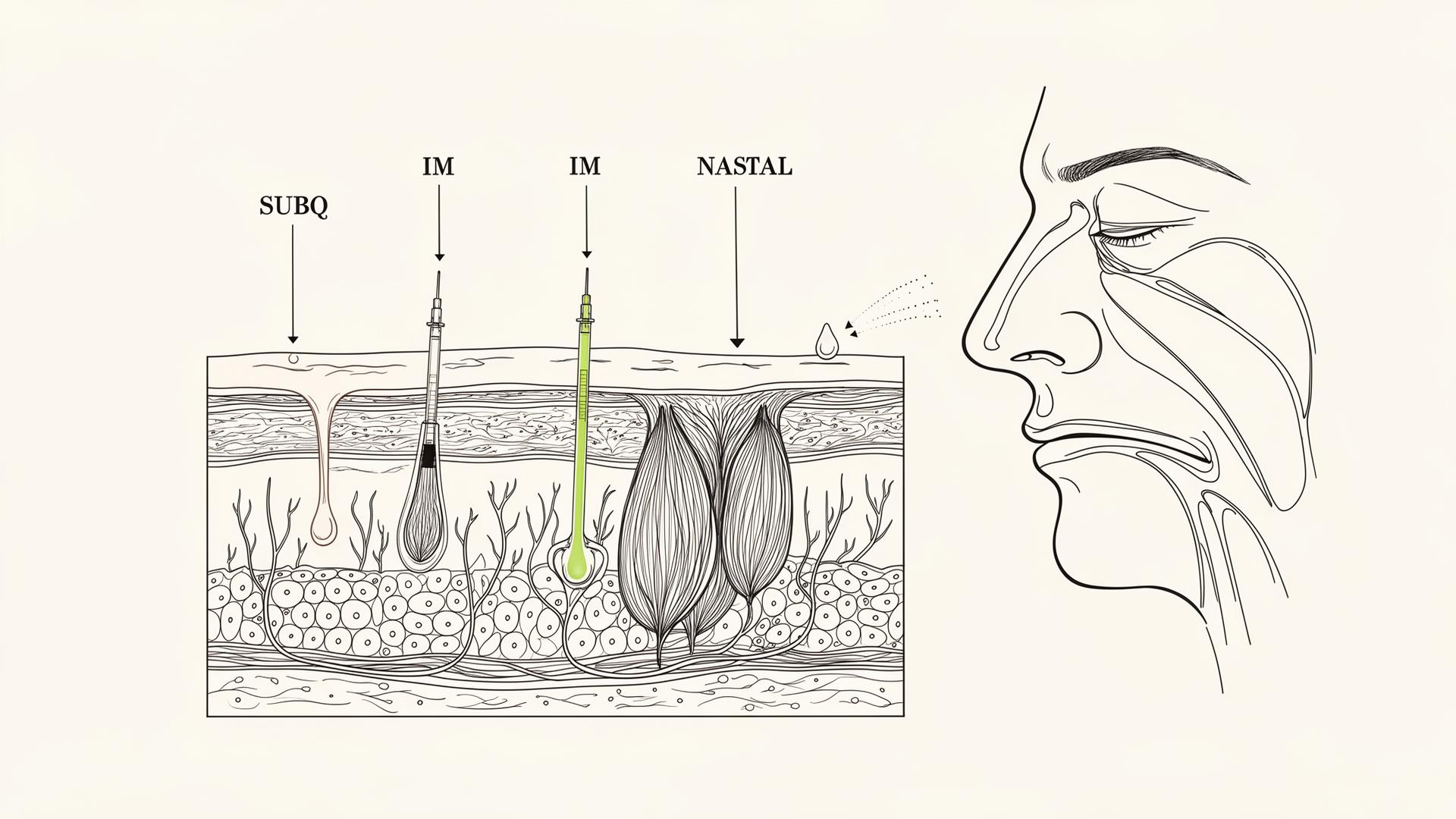
Administration routes: subq, IM, nasal, oral, topical
Subq vs IM vs nasal vs oral vs topical — how the delivery route shapes what a peptide can actually do.
Why route is part of the molecule
Peptides are fragile. Most are destroyed by stomach acid and gut enzymes — which is why injection dominates the category. Some peptides have been engineered to survive oral administration (oral semaglutide / Rybelsus, 5-Amino-1MQ); others work topically (GHK-Cu, KPV) or nasally (Selank, Semax). The delivery route is part of the molecule's identity, not an interchangeable preference. Asking 'can I take BPC-157 sublingually instead of injecting it?' is asking a real question about bioavailability, not a workaround.
Subcutaneous (subq) — the default
Most common route. A short insulin-style needle into the fatty layer under the skin, typically the belly or upper thigh. Lower bleeding risk and easier self-administration than IM. Used for the vast majority of peptides on this site, including BPC-157, ipamorelin, CJC-1295, GLP-1s, melanotan, and PT-141.
Doses are usually small enough to fit on a U-100 insulin syringe, which is what almost everyone in the space uses. See the Reconstitution guide for the math.
Intramuscular (IM)
A longer needle into muscle tissue — usually deltoid, vastus lateralis, or gluteus. Used for compounds with poor subq absorption or specific clinical indications (testosterone esters, B12, some vaccines). Higher discomfort, larger needle, slightly higher bleeding risk. Rarely necessary for the peptides on this site; if a source insists on IM-only without a clinical reason, ask why.
Nasal
Selank and Semax were designed for nasal delivery. The nasal mucosa can absorb small peptides directly into systemic circulation, partially bypassing first-pass metabolism. Bioavailability is lower than injection, so doses are larger and dosing is more frequent.
Quality matters here: a nasal spray is a sterile medical device, not just a bottle. Reconstitute into preservative-containing diluent or use single-day batches.
Oral
True oral peptides are the exception. Semaglutide's oral form uses a permeation enhancer (SNAC) to drag enough drug across the stomach lining; the bioavailability is around 1%, which is why oral doses are far higher than subq doses for the same effect. 5-Amino-1MQ is a small enough molecule to behave more like a conventional drug. Most other 'oral peptide' products on the market are wishful labeling.
Topical
GHK-Cu and KPV both work topically for skin applications — wound healing, hair, inflammation. Topical delivery limits action to the skin itself, which is often exactly what you want. Formulation matters: a copper-peptide serum that is not pH-stable or that is paired with vitamin C will deactivate. Read the formulation, not just the label.
Does subq vs IM injection actually change the effect of a peptide?+
For most peptides, no — the absorption curve is slightly slower from subq but the total amount delivered is similar. For oil-based depots and a few specific compounds (e.g. some testosterone esters), the route does matter.
Why is oral bioavailability so low for peptides?+
Two reasons. First, stomach acid and pancreatic proteases break peptide bonds. Second, the molecules are large and polar, so the gut wall does not absorb them well. Engineering around both is hard — semaglutide's oral form is a notable exception.