Peptides 101: what they are and why everyone is talking about them
A grounded primer on what peptides actually are, how they work in the body, why interest has exploded, and how to think about the category without hype.
What is a peptide, really?
A peptide is a short chain of amino acids — the same twenty building blocks your body uses to assemble every protein you've ever made, just strung together in shorter sequences. Insulin is a peptide (51 amino acids). Oxytocin is a peptide (9 amino acids). The hormone that tells your stomach you're full, GLP-1, is a peptide (30 amino acids). Most of the compounds discussed on this site are synthetic peptides — designed to act on a specific receptor or signaling pathway, then chemically optimized for stability so they survive long enough in the body to actually do something.
The line between 'peptide' and 'small protein' is fuzzy and mostly academic. Biochemists tend to draw it at around 50 amino acids; below that you have a peptide, above that you have a protein. The practical line that matters for users is delivery: peptides are usually too fragile for the gut, which is why subcutaneous injection dominates the category. The exceptions — oral semaglutide, nasal Selank, topical GHK-Cu — were each engineered around that fragility, with permeation enhancers, mucosal-friendly formulations, or copper-binding chemistry that survives where the parent molecule would not.
What makes peptides interesting as a drug class is specificity. A small molecule like ibuprofen interacts with dozens of targets in the body; that's why it has a long side-effect profile. A peptide is shaped like the natural ligand for a specific receptor, so it tends to bind that receptor and very little else. Semaglutide hits GLP-1 receptors and almost nothing else. BPC-157 hits pathways involved in tissue repair and almost nothing else. That specificity is what gives the category its therapeutic promise and what gives it relatively narrow side-effect profiles compared to traditional pharmaceuticals.
How peptides actually work in the body
Most peptides act as signaling molecules. They bind to a receptor on the surface of a cell, the receptor changes shape, and that shape change triggers a cascade of events inside the cell — usually changing which genes get expressed, which proteins get made, or which other signals get released. The peptide itself is rarely the thing 'doing' the effect; it's the messenger that tells the cell what to do.
This matters for two practical reasons. First, peptides don't accumulate the way some small-molecule drugs do — most are cleared from circulation within minutes to hours, broken down by peptidases back into their constituent amino acids. The effect persists because the downstream cellular changes persist, not because the peptide is still floating around. Second, because they bind specific receptors, the dose-response is sharply non-linear: below a threshold, nothing happens; above the saturation point, more drug just means more side effects without more effect.
A few peptides work differently. GHK-Cu binds copper ions and acts more like a delivery vehicle for the metal than a classical signaling molecule. BPC-157 appears to work through multiple mechanisms simultaneously — angiogenesis, nitric oxide modulation, growth factor expression — which is part of why it's harder to study and easier to over-claim. Knowing roughly how a compound is supposed to work tells you whether the claims about it are plausible.
Why the category exploded
Two things converged. First, synthesis costs collapsed. Solid-phase peptide synthesis — the technique that lets a chemist build a custom amino acid chain one residue at a time — went from artisanal laboratory work in the 1980s to highly automated, contract-manufactured commodity production in the 2010s. Sequences that cost thousands of dollars per gram a decade ago now cost dollars. That collapsed the entry cost for both legitimate research and gray-market resale.
Second, a handful of breakout compounds generated enough anecdotal momentum to break peptides out of bodybuilding forums and into mainstream conversation. GLP-1 agonists (Ozempic, Mounjaro) rewrote the obesity treatment landscape and put the word 'peptide' on the cover of magazines. BPC-157 picked up a cult following in CrossFit and combat-sports communities as an injury-recovery tool. Melanotan-II turned into the world's most chaotic suntan product. PT-141 became a real prescription for female sexual dysfunction. Every one of these stories pulled new people into the category.
The information landscape has not caught up. Most users still learn about peptides from podcasts, Reddit threads, and Twitter accounts where the signal-to-noise ratio is brutal, dosing recommendations are copy-pasted with no source, and 'research-use-only' becomes a wink rather than a real constraint. That is the gap this site exists to close.
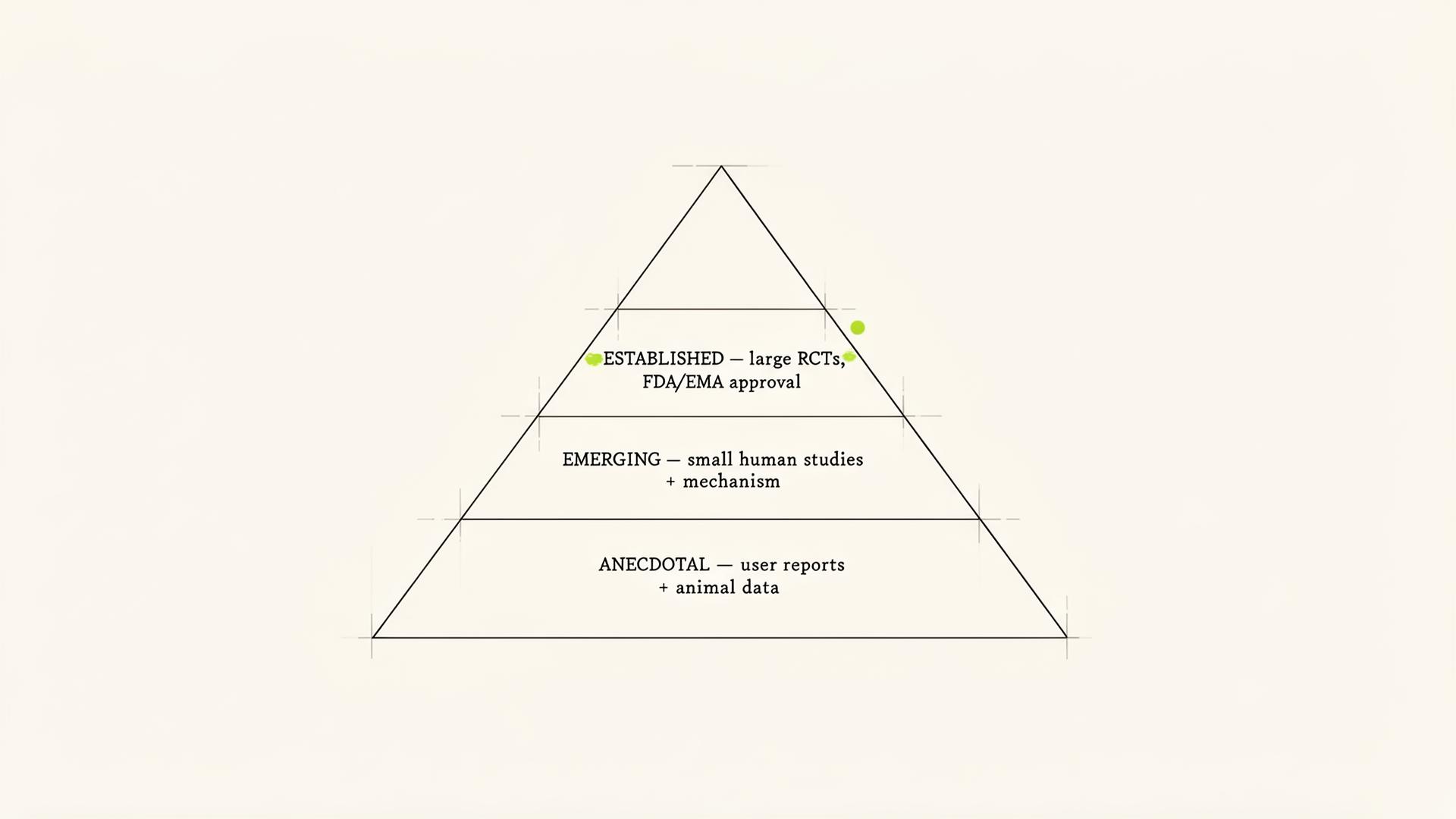
Three evidence tiers — and what they mean for you
We tag every peptide on the site with one of three evidence labels. Calibrating your confidence to the right tier is the single most important habit you can build as a user.
- Established — large randomized controlled trials in humans, plus FDA or EMA approval for at least one indication. The effect size and the side-effect profile are quantified. Examples: semaglutide, tirzepatide, tesamorelin, PT-141.
- Emerging — smaller human studies (often Phase I/II), animal data with a clear mechanistic story, and consistent anecdotal reporting that matches the mechanism. The signal is real but the magnitude is uncertain. Examples: ipamorelin, CJC-1295, GHK-Cu.
- Anecdotal — predominantly user-reported, with animal data and mechanism plausibility but limited or no controlled human evidence. The compound may work brilliantly, may do nothing, or may work for some specific subgroup. Examples: BPC-157, TB-500, Epitalon.
'Anecdotal' does not mean it does not work. It means the data is not there yet. Calibrate your confidence accordingly — be more conservative with dosing, more attentive to side effects, and less surprised when the results do not match a Reddit thread.
Categories you'll see again and again
Almost every peptide on the consumer radar falls into one of five buckets. Recognizing the bucket up front tells you most of what you need to know before you read a single protocol.
- Metabolic / GLP-1 — semaglutide, tirzepatide, retatrutide. Slow gastric emptying, suppress appetite, improve insulin sensitivity. The most heavily studied class on this site by orders of magnitude.
- Growth hormone secretagogues — ipamorelin, CJC-1295, tesamorelin, sermorelin, MK-677. Push the body's own pulsatile GH release rather than replacing GH directly. Used for body composition, recovery, and sleep.
- Healing and tissue repair — BPC-157, TB-500, KPV. Promote angiogenesis, modulate inflammation, accelerate connective tissue repair. Anecdotal-tier evidence but a loyal following in athletic populations.
- Cosmetic / skin — GHK-Cu, Melanotan-II, epithalon. Skin remodeling, pigmentation, photoaging. Topical for skin, injectable for systemic effects.
- Sexual function and neuropeptides — PT-141, Selank, Semax, Kisspeptin. Act on central nervous system pathways for libido, anxiety, focus, or fertility-axis modulation.
How peptides get delivered to the body
Because peptides are fragile and large enough that the gut wall doesn't absorb them well, delivery is part of the molecule. The choice is rarely up to the user — it's baked into the chemistry. The Administration guide goes deep on each of these; the short version:
- Subcutaneous injection (the default) — short insulin needle into the fatty layer of the belly or thigh. Used for the vast majority of peptides on this site. Easy, reliable, low-discomfort.
- Intramuscular injection — longer needle into muscle. Reserved for specific compounds that need it or for clinical indications with depot formulations.
- Nasal — designed for compounds like Selank and Semax. The nasal mucosa absorbs small peptides reasonably well and partially bypasses first-pass metabolism.
- Oral — the exception, not the rule. Oral semaglutide and 5-Amino-1MQ are engineered around the bioavailability problem. Most other 'oral peptide' products are wishful labeling.
- Topical — GHK-Cu, KPV, and certain copper peptides act locally on the skin. Formulation chemistry matters more than dose.
Legal status, in one paragraph
Most peptides in active use are sold as 'research compounds' rather than as approved drugs. A few — semaglutide, tirzepatide, tesamorelin, PT-141 — are prescription medications with full FDA approval for specific indications. Compounded versions of GLP-1s have existed under FDA shortage provisions; the FDA has actively narrowed those windows since 2023, so the legal status of compounded semaglutide and tirzepatide is now a moving target. Outside the United States, rules vary widely. Source carefully, never assume a product is what its label says without third-party verification, and read the Legal Status guide before you start ordering anything.
If you're brand new — start here
There is no shortcut, but there is an order of operations that prevents the most common mistakes. Roughly:
- Pick one outcome you care about. Not three. Not a stack. One.
- Use the Finder to see which peptides target that outcome and what the evidence tier looks like.
- Read the deep-dive page on the peptide you land on. Read the Dosing Fundamentals guide and the Reconstitution guide before you order anything.
- Talk to a peptide-literate clinician. The Working With a Clinician guide explains what that means and how to find one.
- Start with the published low-end dose, not the bro-dose your favorite podcaster mentioned. Titrate up only if the low dose is well-tolerated and clearly subtherapeutic.
- Track one or two measurable outcomes — weight, recovery time, sleep score, libido — so you have actual data when you decide whether to continue.
Are peptides legal in the United States?+
It depends on the molecule. FDA-approved peptides like semaglutide, tirzepatide, tesamorelin, and PT-141 are legal with a prescription. Most others are sold as research-use-only compounds and are not approved for human consumption. The Learn → Legal status guide covers this in detail and is the right place to look before ordering.
Are peptides the same as steroids?+
No. Anabolic steroids are synthetic androgens that bind the androgen receptor directly to drive muscle and tissue growth. Peptides are short amino-acid chains that act on a much wider range of receptors — growth hormone, melanocortin, GLP-1, opioid, and others — and most of them have nothing to do with the androgen axis. They are pharmacologically distinct categories with different mechanisms, different side-effect profiles, and different legal statuses.
Can I take peptides orally?+
A few, yes — semaglutide has an oral formulation (Rybelsus) that uses a permeation enhancer to drag the drug across the stomach lining, and 5-Amino-1MQ is small enough to behave like a conventional oral drug. Most peptides are degraded by stomach acid and gut enzymes within minutes, which is why subcutaneous injection is the default route. See the Administration guide.
How long does it take to feel a peptide working?+
It varies dramatically by class. GLP-1s for appetite are usually noticeable within the first week of dosing. GH secretagogues like ipamorelin take 4–8 weeks for body composition changes but improve sleep within days. BPC-157 for an injury is typically a 4–6 week window. PT-141 acts within hours. The Class guides give specific timeline expectations.
Do I need a doctor to use peptides?+
For FDA-approved peptides — yes, you need a prescription, full stop. For research-use peptides, there is no legal requirement, but it is strongly recommended. A peptide-literate clinician can order baseline bloodwork, monitor for side effects, and catch contraindications that you won't. See the Working With a Clinician guide.